Research and innovation
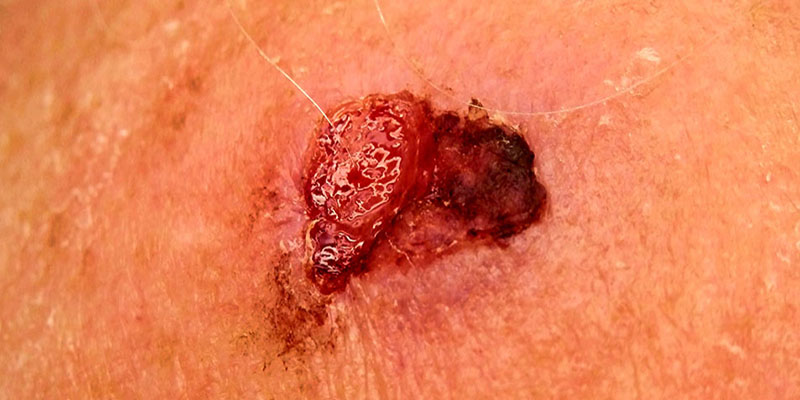
Dr Magnus Lynch is passionate about advancing our understanding of skin cancer through cutting-edge research. His work spans from pioneering spatial mapping of cell populations in skin cancers like basal cell carcinoma to investigating the potential of imaging technologies such as Optical Coherence Tomography, and understanding weaknesses in machine learning systems for skin cancer detection. His earlier research uncovered how spatial dynamics influence the behaviour of mutant cells in the skin, shedding light on the earliest stages of cancer development. He has also led a clinical trial exploring the potential for non-invasive diagnosis of melanoma through epigenetic profiling of the skin surface. Current work in the lab focuses on 3-dimensional cell culture models of skin cancer.
SELECTED SKIN CANCER RESEARCH PUBLICATIONS:
Ganier C, Mazin P, Herrera-Oropeza G, Du-Harpur X, Blakeley M, Gabriel J, Predeus AV, Cakir B, Prete M, Harun N, Darrigrand JF, Haiser A, Wyles S, Shaw T, Teichmann SA, Haniffa M, Watt FM, Lynch MD. Multiscale spatial mapping of cell populations across anatomical sites in healthy human skin and basal cell carcinoma. Proc Natl Acad Sci, 2024. Pubmed ID: 38165934
Lynch MD. Beyond the algorithm: Ethical Challenges in AI-Driven Skin Cancer Diagnosis. British Journal of Dermatology, 2024. DOI: 10.1093/bjd/ljae490
Hughes S, Srenathan H, Lynch MD (Joint senior author), Leeman H. Multi-center experience from tertiary skin cancer units on the role of Sentinel Lymph Node Biopsy in patients with pT1b melanoma. Clin Exp Dermatol, 2023. Pubmed ID: 38112606
Wan B, Ganier C, Du-Harpur X, Harun N, Watt F, Patalay R, Lynch MD. Applications and future directions for Optical Coherence Tomography in Dermatology. British Journal of Dermatology, 2021. Pubmed ID: 32974943
Du-Harpur X, Arthurs C, Ganier C, Woolf RT, Laftah Z, Lakhan MK, Salam A, Wan B, Watt FM, Luscombe NM, Lynch MD. Clinically-relevant vulnerabilities of deep machine learning systems for skin cancer diagnosis. Journal of Investigative Dermatology, 2020. Pubmed ID: 32931808
Lynch MD, Lynch CNS, Craythorne E, Liakath-Ali K, Mallipeddi R, Barker JN and Watt FM. Spatial constraints govern competition of mutant clones in human epidermis. Nature Communications, 2017. Pubmed ID: 29066762